Mango

Mango! is the websites own resident cat. Born in Norfolk, United Kingdom in 2019 at the Cat's Protection League Dereham Centre. The Cats protection league at the time named Mango after his mum who had 4 kittens. Mango was named as Mango K4.
He was adopted at about 10 weeks old by his owners and, at the time, had 3 Sisters (Simba, Diamond and Molly) and an older brother, Sammy.
He looked towards Sammy as his role model!
Unfortunately Sammy Died, followed by Molly and Mango had to step us as the male cat of the household.
He loved his role and quickly developed into a nice boy cat who was and still is loved much by his owners.
He often played with Simba, but less so with Diamond who is a shy and independent cat who looked to avoid Mango as much as possible.
Illness
Mango adored his young female owner, and one day she noticed something unusual—his pupils were different sizes. One was significantly larger than the other and didn’t respond to changes in light. Naturally, this raised concern.
By the next day, however, both pupils had returned to normal. The owners assumed it was a temporary reaction, possibly triggered by something Mango had eaten.
Unfortunately, this was only the beginning of Mango’s health troubles. Soon after, he developed a pronounced head tilt and struggled to walk without stumbling. His eyes began darting rapidly from side to side. Suspecting an inner ear infection affecting his balance, the owners took him to the vet.
The initial examination didn’t reveal anything alarming, and Mango was prescribed antibiotics. When his condition failed to improve, a second vet visit was arranged. This time, a swab was taken from Mango’s ear, revealing a rare bacterial infection.
Mango was diagnosed with both Staphylococcus and Acinetobacter—a highly unusual combination that wasn’t responsive to the initial antibiotics. A new course of treatment was started, including intermittent corticosteroids and marbofloxacin.
Mango began to show signs of recovery, and the medication was eventually stopped. Sadly, his health deteriorated rapidly afterward, prompting yet another vet visit.
To get to the root of the issue, the vet recommended an MRI scan—costing around £2,000. With no real alternative, Mango was referred to a specialist vet clinic located 100 miles away.


Mango was seen by the Vets and following the scan and detection of the infected tissue an operation was required - that he survived :-), the hospital report is below (this is a big read but if you have a cat with these symptoms then please look at this story, it will hopefully give you hope your cat too can be successfully treated :-) :-
History:
Mango presented with a two-month history of a waxing/waning right sided head tilt, nystagmus, right vestibular ataxia
and lethargy. Mango had a culture and sensitivity performed of material from the right ear which was reported to
reveal a mixed Staphylococcus and Acinetobacter infection which was reported to be susceptible to marbofloxacin.
Mango has been on intermittent corticosteroids and marbofloxacin over the last two months which he tends to
respond to. These medications were stopped a week ago, and two days after cessation of the medications Mango
showed a worsening of lethargy, a right sided head tilt and right vestibular ataxia. Mango has not wanted to eat or
drink as normal.
General physical examination:
On physical examination Mango had a heart rate of 188 beats per minute with strong synchronous pulses. The
mucous membranes were pink and capillary refill time was 2 seconds. Mango had a respiratory rate of 20 breaths per
minute and thoracic auscultation was unremarkable. Abdominal palpation did not reveal any abnormalities. The
peripheral lymph nodes were within normal limits. The rectal temperature was 38.1̊C. Mango weighed 3.3kg and had a
body condition score of 4/9.
Neurological examination:
- Mentation: quiet but responsive
- Posture/gait: right sided head tilt with marked right vestibular ataxia
- Postural reactions: absent paw positioning in the right thoracic limb and right pelvic limb, intact in the left thoracic and left pelvic limb
- Segmental spinal reflexes: intact withdrawal, patella and perineal reflexes
- Cranial nerves: absent palpebral reflex OD, absent menace response OD; otherwise unremarkable
- Palpation: comfortable on spinal palpation Neuroanatomical localisation: right vestibular syndrome with intracranial involvement and right facial nerve paralysis
Differential diagnoses included otitis/media interna with intracranial extension, neoplasia, other inflammatory/infectious
Diagnostic investigations:
-Haematology and biochemistry profiles: hyperglycaemia 14.3mmol/l (3.9-6.6); mild hyperglobulinaemia 55g/l
(20-45), otherwise unremarkable
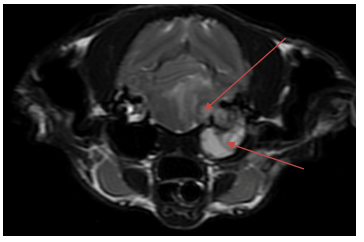
- MRI of the Brain:
- Right otitis externa, media and interna with lesion extending into the calvarium and affecting the local
meninges. These changes likely represent an infection with mild otitis externa and severe otitis media
and interna which extended intracalvariarly with the formation of an intracalvarial abscess/granuloma.
A concurrent polyp or cholesteatoma cannot be fully excluded. - Foramen magnum herniation secondary to increased intracranial pressure
- Mild perilesional oedema
- Possible right CN VIII neuropathy
- Equivocal muscle atrophy of the digastricus muscle
- Phlegmon/fascititis (sterile vs septic) and focal myositis of the right caudoventral right pterygoid muscle
- Mild right medial retropharyngeal lymphadenopathy likely reactive
- Serology for Toxoplasma gondii (referral vet): negative
- Ophthalmologic examination: two small superficial ulcers present OD
- Culture results (from surgery): results pending
Hospitalisation
Presumptive diagnosis: otitis media/interna with intracranial empyema
Mango was hospitalised with us from the 10th October until 15th October. Neurolocalisation was consistent with a right
vestibular syndrome with central involvement and facial nerve paralysis. MRI revealed a right otitis media/interna with
extension into the cranial cavity causing an intracranial empyema causing signs of increased intracranial pressure
(foramen magnum herniation). Mango was started on mannitol, IV antibiotics (Marbofloxacin based on previous culture
results) and low dose corticosteroids. Over the next 48 hours Mango showed some improvement in his mentation and
remained cardiovascularly stable. We discussed management options including performing a ventral bulla osteotomy
(VBO), vs continued medical management alone (antibiotics).
The prognosis of cats with intracranial empyema/abscessation can be good, however the long term median survival
time can be quite variable. The marked changes on MRI in Mango’s case are concerning and there is the risk of
sudden deterioration, or relapse of clinical signs. Mr and Mrs Doubleday elected to proceed with a VBO and this was
performed on the 13th October (see separate surgery report). Mango was hospitalised post-surgery and on discharge
Mango was bright, showed mild right sided head tilt and improved/occasional vestibular ataxia. We have
recommended a long course of antibiotics (minimum 8 weeks) and will continue to assess Mango’s response to
therapy. We have asked for a re-examination in three weeks’ time, or sooner if there are any concerns.
Mango had a tarsorrhaphy performed whilst under general anaesthesia and a contact lens placed to help protect the
right eye. We would plan to remove these sutures in 3 weeks’ time at the time of re-examination.
Medication (adjust as necessary):
- Marbofloxacin (Marbocyl) 5mg tablets: give TWO (2) tablets, orally, ONCE daily for at least eight weeks
- Prednisolone 1mg tablets: give ONE AND A HALF tablet once daily until 20th October, then 1 tablet once daily until
next recheck
- Lubrication (eye): apply in both eyes every 4-6 hours
Two Days after his operation Mango was discharged with the following advice:-
Wound: please check the wound twice a day and contact us if it becomes red, swollen, starts to discharge or open up. Mango must wear a buster collar at all times if he tries to scratch at the wound until the wound is all healed/until it has been re-examined in 12-14 days’ time as detailed below.
Exercise: Mango must be strictly rested for the next 2 weeks to allow the internal stitches to heal. Please keep him restricted to a large dog crate with a litter tray, water bowl and bedding. After two weeks he can be allowed access to a small room where there is minimal furniture for him to jump on/off for the next 4-6 weeks. He should not be allowed to run, jump, climb the stairs or play excessively during this time.
Monitoring: please contact us if Mango becomes lethargic, goes off his food, has vomiting, passes diarrhoea or you have any other concerns. It is possible that Mango may develop a seroma (sterile fluid swelling) at his wound site. This should resolve with rest. Please contact us if you have any concerns.
Follow up: Please make an appointment with your vet, 12-14 days after surgery to have Mango re-examined and the wound checked. Sutures are absorbable and do not need removing. We will be in touch with his culture and histology results.
Medication: Please follow the medication instructions on the separate Neurology report.
Discharge

Recovery
After 2 weeks of a lot of sleeping Mango went to the vets for follow up and although he had (and still has) a very slight head tilt he was virtually fully recovered and much happier, lively and only minimal problems with walking when he was surprised.
Mango was fully discharged!!!!!
